


Forum Conversation: Norman Fenton
On The Revelations of Pandemic Data


In an exclusive interview with the Forum, Norman Fenton, a veteran UK risk management professor and mathematician explains how the manipulation of pandemic data by scientists, government agencies and mainstream media supports a false narrative with devastating consequences.
By David Marks
Forum: Norman Fenton, welcome to the Forum Conversation. The analysis you’ve done over the last few years gives incredible insight into what actually unfolded during the pandemic. Before we discuss those findings, can you help us understand how you apply your knowledge to evaluating information outside of your area of expertise, including medical data?
Fenton: For many years I’ve collaborated intensively with clinical experts in different medical domains. For example, before the COVID crisis, I was the principal investigator of a large project funded by the United Kingdom Engineering and Physical Sciences Research Council. Our group uses Bayesian statistical methods, where available knowledge and expertise are combined with data to help improve decision-making for prognosis and diagnosis of chronic medical conditions.
We analyzed data for specific conditions such as rheumatoid arthritis, diabetes, chronic heart failure, pelvic floor syndrome, multiple sclerosis, and worked with the clinicians to determine causal explanations for observed data so that they can be incorporated into our decision-support systems. So, for example, in the area of trauma we collaborated with surgeons to help improve the decision-making parameters for whether or not to amputate a limb.
For these types of analyses there aren’t massive relevant databases, which is why you need to combine the relatively small amount of available data with the perspective of experienced clinicians. We work with them to build frameworks for effectively eliciting the knowledge needed to make sound decisions. Practical causal models are designed that can be populated with the raw data that we have available, which then provides guidance for those involved in healthcare procedures.
We rely on clinicians for checking all aspects of analysis. Although we have worked with pathologists and epidemiologists in understanding the numbers, information about the COVID pandemic doesn't require a lot of medical knowledge. What was more important was that using only publicly available data enabled us to expose many crucial flaws in the COVID narrative pushed by governments and the mainstream media.
Forum: How did you apply Bayesian analysis to understanding the initial data about testing for the COVID virus?
Fenton: A good example of how we used Bayesian analysis was to answer the question: Do I, or do I not, have the SARS-CoV-2 (COVID) virus? And specifically, if I'm asymptomatic, what is the probability that I might have the virus? Answering this question correctly was the focus of one of our first inquiries.
Suppose that at a given time there is data available suggesting that, in the general population, one in a thousand asymptomatic people were likely to have the virus. Such data was never confirmed of course, the infection rate varied over time, but I will use it to explain the Bayesian reasoning.
If I take a PCR test and it’s positive but I’m not feeling ill, I would want to know if I really have the virus. In other words, if I am one — of the one-in-a-thousand people — who is asymptomatic but carrying the virus, I’d want to know the accuracy of the test. There weren’t any reliable studies about the reliability of the PCR test, but the public was assured these tests were very accurate. Let’s suppose there was only a one-in-a-hundred chance that someone who doesn't have the virus will test positive — a 1% false positive rate. Then conversely, if I don't have the virus, there's a 99% chance of a negative test. With this information most people assumed if you tested positive you almost certainly had COVID. But that is not the case.
Think about a group of 10,000 asymptomatic people getting tested. Because we are assuming one-in-a-thousand asymptomatic people have the virus, that means about 10 of the 10,000 really have the virus. Let’s also assume these genuinely infected people test positive. Then we are left with just under 10,000 people — 9990, who do not have the virus. But a PCR test with only a 1%false positive rate still means that about 100 of these people would falsely test positive. So in total there are 110 people testing positive of whom we know only 10 will actually become ill from the virus. So, the actual probability that you've got the virus if you test positive is closer to 10%. This means that with reasonable assumptions about the underlying infection rate and test accuracy, the PCR test used as a standard for life-impacting decisions and mandates, had a 99% inaccuracy rate for asymptomatic people testing positive.
The confusion lies with the incorrect assumption that even if you don’t have symptoms of the virus, that the possibility of a false positive in the PCR test is only 1%. As more accurate calculations based on reliable data show, that is clearly not the case. To assume these probabilities are equal is known as the fallacy of the transposed conditional. In the courtroom, when DNA evidence is misinterpreted, it’s called the prosecutor's policy. Those contradictory figures should have raised important questions — it’s not that complicated — it can be presented in a confusing way, but scientists who knew better ignored this data.
Forum: Have the results of that comparative data been confirmed by other studies?
Fenton: We looked at the numbers from a study at Cambridge University where they tested several thousand asymptomatic students for the virus over weeks using pooled PCR testing. And during that period what they found was that very few students tested positive. In fact, over the period, only 43 of the 10,394 tests were positive.
However, unlike what happens in PCR testing in the general population, they did a second confirmatory test on each of the same samples that tested positive. They applied this more reliable, approved standard, where two positives were needed for confirmation; if either one was negative, it meant nobody in the pooled sample was infected. They found 36 out of the 43 samples that had tested positive, when re-tested afterwards, showed negative. So, what they saw was 84% of asymptomatic students showing a positive result on the initial test didn't have the virus, confirming a very high inaccuracy rate.
Forum: What was the response to your analysis of the Cambridge study? It should have had some impact on policy.
Fenton: We modeled the data properly and were able to get better predictions about the false positive rate and the true underlying infection rate across the asymptomatic population. We wrote a report, vigorously reviewed by our colleagues in data analysis, and then sent it out to various medical publications. We were shocked that it didn't get to the review stage in any journal. It was the first of our reports rejected with claims that there was insufficient interest or because it was not in their scope. Our analysis of the Cambridge study was even rejected by preprint servers, who have the most tolerant standards, normally publishing anything that isn't plagiarized.
Forum: This must have been extremely frustrating. How did you account for this unreasonable response?
Fenton: No one wanted to admit or expose that a very significant proportion of asymptomatic testing yielded false positives. Some people simply claimed they knew that what we saw couldn't be true because they were absolutely sure that the false positive rate of the PCR test is less than 1%. They didn’t want to look at that in the context of what we demonstrated because it contradicted the original driving narrative of the COVID pandemic. Their beliefs were based on a fallacy that drove all pandemic policies.
We can see there was an effort to show an exponential increase in case numbers. The simple extrapolation from what we had shown was that if you test more people — especially a lot of more asymptomatic people — you’ll seem to show more cases, many that actually were false positives. This wouldn’t have helped the arguments for lockdowns, mandates, and later for vaccines. When lockdowns were easing and people were going back to work who were perfectly healthy and didn't have any symptoms — they still had to get PCR tests. Then again, you have all of the subsequent limiting policies and insistence on vaccination based on what was another huge percentage of false positives.
Forum: There seemed at the beginning of the pandemic a rationale for testing and consideration of how to best protect the public. The media showed body bags on the streets of China, with the implication that if something wasn’t done, this would happen everywhere.
Fenton: We did some appropriate analysis and looked at the infection fatality rate; what the probability of dying was if you contracted the COVID-19 virus. The infection rate and fatality data were gathered from all of the public studies that were available.
We then did a meta analysis, putting all available data together, taking into account that in the early weeks of the pandemic it was mostly the seriously ill, hospitalized patients who were getting the PCR test; and so they were the largest group confirmed as COVID cases. It was obvious how the numbers were being reported incorrectly. If the majority of people with confirmed COVID cases are in hospitals, then the probability of dying with COVID will seem much higher than it actually is, because you're focusing on a restricted group. This finding uses common sense, not sophisticated data analysis.
Our work concluded that the infection rate — the proportion of people infected — was higher than being presented. But crucially, the infection fatality rate, the possibility that you would die if you were infected with the virus, was much lower than was being reported. Over time, accurate fatality rates only confirmed our work and the conclusions of other studies. The mortality rate was never that high and mostly among those with other pre-conditions. But again, this work was virtually ignored.
Forum: Governments and health authorities admitted that having preexisting conditions put those patients in the highest risk group for hospitalization and death. How did you take that into account?
Fenton: We gathered very good data on this. Through requests based on freedom of information we have indisputable numbers for the UK from over the first two years. And out of 136,000 deaths formally classified as from COVID on their death certificates, about 5000, only 5%, didn't have at least one other comorbidity. In this group, there were only three children under the age of 20.
There's another study which looked in detail at the hospital records of all children who entered an ICU with COVID in the first year of the pandemic — about 250 — it was a lower number than a typical flu year. And when they started to examine the numbers, it turned out, there were 38 of those children who ended up dying. Eight of those had their death attributed to COVID — the others were children who had a positive PCR test, but were admitted to the ICU with symptoms of a very serious condition like cancer. And of the eight whose death was attributed to COVID, at least seven had preexisting life-threatening conditions. So essentially, they showed that children under the age of 20 in the UK who died with COVID, actually died from something else. At least in this analysis from the first year, the risk for young people dying from COVID approaches zero.
Forum: Has there been analysis of the figures comparing the percentage of those dying in previous years with the flu and a comorbidity, compared to similar COVID-19 statistics?
Fenton: It is interesting that once COVID-19 started, a lot of the flu data, which had been previously easy to find, suddenly became hard to locate or unavailable. We attempted to get that information without much success, as it would've been a very good comparison. There's certainly anecdotal knowledge. It has always been that the elderly often die with complications of the flu or pneumonia, and it is one of the reasons that they have been considered a high-risk group with COVID.
There was a genuine excess death peak in February and March of 2020, when COVID first arrived. We're now finding out that was actually due to very poor medical decisions made in respect to the elderly. And I'm not just talking about giving the wrong treatments, such as inappropriately putting patients on ventilators. My clinical colleagues now realize that moving hospitalized elderly patients into care homes where COVID spread like wildfire was catastrophic. The subsequent increase in deaths from the novel COVID virus were likely connected to mismanagement and lack of appropriate treatment.
Forum: Does the data reveal whether the COVID-19 virus actually was more dangerous or deadly, or that as the pandemic went on, it became increasingly so?
Fenton: It appeared dangerous at the beginning, and we still don’t know how much of that was manufactured or due to the catastrophic mismanagement of the elderly. I can’t be certain about early on, but there are very strong indicators that the so-called, subsequent massive waves were greatly exaggerated. For example, in the UK, the second wave, which began in the winter of 2020, was supposed to be much worse in terms of COVID case numbers and fatalities than the first wave.
Again, here it’s important to not just look at numbers, but understand the source of those figures. If you only consider the UK government COVID dashboard, which only issues details of COVID case numbers, hospitalizations and deaths, and recognize they are still dependent on the PCR test, you see a much bigger peak than the first wave. This data was used repeatedly to warn us of the return of deadly conditions.
We looked at other important, independent indicators in the UK. The National Health Service COVID triage dashboard monitored the emergency calls and responses specifically for patients with COVID symptoms. These are people who are forced to call emergency services and get an ambulance because they've got worsening COVID symptoms. The numbers reflect genuine healthcare emergencies rather than questionable test results.
That graph clearly shows earlier in 2020 when the virus first hit, there were genuine peaks. But in the winter of 2020 through 2021, there are only ripples of increased emergency calls very similar to a normal flu season.
So there was an initial increase, which can be accounted for by a new powerful variant of the flu that was mismanaged. But the increasing scale claimed by governments can’t be substantiated, and the additional data from the COVID triage dashboard contradicts those inflated figures.
Inadequate and flawed trials
Forum: Can you help us understand what you see as the central flaws of the vaccine trials?
Fenton: I have never run a clinical trial. I've only looked at data on clinical trials, so I'm not a clinical trials expert. My experience and expertise is mostly in judging results of observational trials. But there were many obvious problems with the main Pfizer vaccine trial that are just being revealed.
The Pfizer trial was the basis for the 95% effectiveness claim that enabled emergency use authorization for the vaccine. As with all randomized controlled trials it was supposed to be a double blind, placebo-controlled trial. In one of the largest in Argentina, they had an equal number of uninfected patients getting a vaccine or the placebo; 22,000 received the COVID vaccine and 22,000 got a saline injection. Now we know there were all kinds of protocol violations, including people in the placebo group finding out they hadn’t been vaccinated.
A significant number of them dropped out or were given the vaccine. The 95% effectiveness claim was based on the fact that post injection, there were 162 COVID cases among placebo participants compared to just eight among the vaccinated participants. But a much larger number of suspected but unconfirmed cases were fairly evenly spread among those in the vaccine and placebo groups. And a disproportionately small number of vaccinated participants with symptoms received PCR tests compared to placebo participants with symptoms.
Pfizer also excluded participants who developed COVID before their second dose. There were 143 such patients withdrawn. Many of the irregularities occurred at one site in Argentina that had the largest number of participants, almost all of whom were recruited close to the deadline. It is also important to note that no safety outcome was tested in the trial, and to date, more deaths have been recorded overall in the vaccine arm than in the placebo arm.
Not just in Argentina, but in many of the big observational trials conducted after the vaccine rollout, anyone who was vaccinated and who got COVID within two weeks, was classified as an unvaccinated person. The biased rationale behind this decision was that it takes at least two weeks for the vaccine to take effect. This misclassification became accepted as a worldwide practice that distorted the data everywhere.
So, in these observational trials, you’ve got this unbelievable bias in the data, right from the start. Added to that, we know that as in the Pfizer trial, in observational trials a disproportionately small number of vaccinated people did not get routinely tested compared to those who were unvaccinated. Everything done was to justify vaccine rollouts and give subsequent doses.
Forum: Did the pharmaceutical trials combine the results from a number of different countries, adding them all together? And if the Argentinian figures had been removed, would the results have been less conclusive?
Fenton: The Pfizer trial wouldn't have reached the target without the Argentine site, where there had been mass recruitment just before the deadline. There's circumstantial evidence that it was set up to obtain the 95% effectiveness figure.
Forum: Fairly soon after these inflated claims of effectiveness, we heard about so-called breakthrough cases. That term seems to have disappeared almost as quickly as it arrived, because it became apparent that all cases are breakthrough cases.
Fenton: They sold us a lie. They told us that if you took the vaccine, you wouldn't get COVID and you couldn't transmit it. Now we are finding out that it's the people who received the vaccine multiple times who are getting COVID more than once, rather than the unvaccinated. We've got the numbers showing that in each age group; the vaccinated are disproportionately more likely to get COVID than the unvaccinated.
Forum: The definition of vaccinated has changed over the pandemic. How has that affected data assessment?
Fenton: Despite the shifting definition of the term, we do have data that divides the groups by the number of shots from none to five. The concerted effort to minimize the number of vaccinated people who get COVID was unstoppable. It’s now widely admitted that the vaccine doesn’t stop transmission, confirming actual statistics showing all other analysis was based on skewed results. But when vaccines were being promoted, those of us with expertise who contradicted the interpretation of data were marginalized or ignored. The narrative was framed around an illogical insanity that was widely accepted.
Number of vaccinated people inflated to marginalize the unvaccinated
Forum: There is still an effort to swell the numbers of people who are vaccinated. Is this overt attempt to marginalize the unvaccinated also based on incorrect data?
Fenton: The true proportion of people who are unvaccinated matters in a major way. The Office of National Statistics [ONS] here in the UK made a bizarre claim that in May 2022 only 8% of the adult population is unvaccinated — those never having had one shot. We know that's not true because the UK Health Security Agency has more reliable data that says it’s closer to 20% of adults in the UK who are unvaccinated; and that’s a conservative number. It may be closer to 30%. When you use this higher figure for unvaccinated, you have a more accurate sample of the population, and in every age group we see that there are more COVID cases among the vaccinated.
Forum: How do you know that the UK Health Security Agency figures are more reliable?
Fenton: Firstly, the ONS data is based on a very unrepresentative subset of the UK population. It only includes people who were both counted in the 2011 census and were also registered with a general practitioner in 2019. That categorizing reduces the adult population of England to from about 49 million to about 39 million. So you're missing about 10 million adults. This also assumes the census is correct; better estimates would put that missing population at closer to 16 million, a massive number. And a substantial proportion of those in this missing group are certainly unvaccinated.
Even ignoring the children who were born after 2011, you’ve got a huge influx of immigrants coming in. And then those who aren't registered with a general practitioner are not being pressured by their physician to get vaccinated. It’s overtly a biased sample and not representative.
The UK Health Security Agency is basing their data entirely on the National Immunisation Management Service, which is supposed to have a record of every vaccination, including for COVID. This data can be problematic because it overcounts due to duplicate records — but it doesn’t have a bias that would find lower unvaccinated numbers. From their figures, in May 2022 just under 20% of the adult population was unvaccinated.
Forum: Have these figures been compared publicly?
Fenton: The BBC produced a documentary recently called “Unvaccinated.” They used the ONS figure of 8% of the adult population, presenting this small group as strange outliers who needed to be convinced of their ignorance. Interestingly, the producers contradicted themselves by revealing that to understand attitudes to the vaccines, they had used the ICM survey commissioned by the public broadcaster STV. This was the largest detailed survey about the COVID vaccination program that had been done in the UK. This sampling showed that of 2570 people, 664 were unvaccinated — nearly 26% — which exceeded all other estimates. But the program had a point of view that couldn’t tolerate doubt.
Whether you are a classical statistician or want to do a Bayesian analysis, whichever way you crunch the numbers, the results show a higher population of unvaccinated people than the mainstream narrative suggests. Any analysis of cases or effectiveness changes dramatically when accurate numbers are used.
COVID-19 vaccines don’t work
Forum: The vaccines were promoted as effective in stopping cases. Data and studies that showed the opposite were ignored, although now it has been admitted that the COVID vaccine has never been shown to decrease transmission.
Fenton: What is far worse, there is data that indicates higher vaccination is related to higher rates of infection. A Freedom of Information Act request to the Nova Scotia government in Canada released data that was charted by Jessica Rose. It made this very apparent connection.
Forum: Another country where you compared vaccination and the number of COVID cases was Germany. What did you see there?
Fenton: One argument defending COVID vaccines is that it’s difficult to compare numbers across countries that have very different cultures and healthcare systems. This is partially true, but looking at Germany and its individual states, where they’ve got the same regulations and everybody's equally encouraged to take the vaccine, this is not a factor.
We compared data from Germany over seven days on COVID cases and COVID vaccine uptake rates. Regional differences in the proportion of people vaccinated could be analyzed. For example, in parts of former East Germany there is more skepticism of the government and we saw much lower vaccine uptake rates.
For each region, when you plot the density of cases against vaccine uptake, you get this remarkable correlation whereby the dense case regions are also the dense vaccine uptake regions. And where there are very few COVID cases you have the least vaccine uptake.
Berlin in particular, shows this very clearly; there’s a much higher proportion of the population vaccinated than other areas, over 62%. And it's the hotspot for COVID cases. Of course this data uses numbers based on confirmed cases with testing, and as I've said, I’m skeptical about testing. Nevertheless, it's quite a phenomenal finding that’s virtually ignored.
COVID-19 vaccines and mortality
Forum: The emphasis in public pronouncements shifted to how vaccines limit hospitalization and death. Was that ever looked at in studies?
Fenton: Again this is not a complicated analysis. When you plot the vaccination rate for any given country against the COVID mortality rate there is an obvious trend. If the vaccines were working, what we should be seeing is that countries with higher vaccination rates should have lower COVID mortality rates.
What you actually see is the countries with the lowest COVID mortality rates are essentially the African countries with very low vaccination rates. Now the average population age in African countries is lower than elsewhere, so this is a factor, but even among highly comparable countries, those which have high vaccination have higher mortality rates. Australia, for example, currently has the highest COVID mortality rate in the world and claims 96% are vaccinated. There are variables, but there is certainly no correlation showing that vaccinated populations have a lower chance of dying from COVID.
Forum: Yet the number of cases, hospitalizations and death still drives the narrative, even as the pandemic recedes.
Fenton: Despite obvious issues with how numbers are gathered and analyzed, the case rates are still driven by testing that either is unreliable or applied to a narrow group of patients. Either way, the more testing you do, the more cases and hospitalizations you find; and of course, the more deaths you'll classify as COVID. As cases are massively inflated, subsequent data is useless. Hospitalizations and deaths are real, but many of the COVID cases aren’t. And as has been apparent to anyone who cares to look, most of those who actually have COVID and die are not dying of COVID, they are dying with COVID.
We recognized early on that there was so much manipulation of information that we had to start looking at figures that couldn’t be skewed.
Forum: Your group was one of the first to look at all cause mortality and you recognized some interesting anomalies.
Fenton: Yes, if you want to really understand the safety of the vaccines, you need to analyze all-cause mortality. When we first looked at the ONS data for the UK vaccine program we saw a very strange correlation.
Incredibly, according to the ONS data, as the vaccines were released, there was a significant increase in deaths from other causes than COVID among the unvaccinated. These two statistics should be unrelated. The most likely explanation for this anomaly was that many of those who were dying shortly after vaccination were being classified as unvaccinated. Once the data are adjusted for this misclassification there is no evidence that the vaccines reduce all-cause mortality; rather, there is evidence it may cause an increase, especially in the younger age groups. This should have caused great concern and immediate intervention.
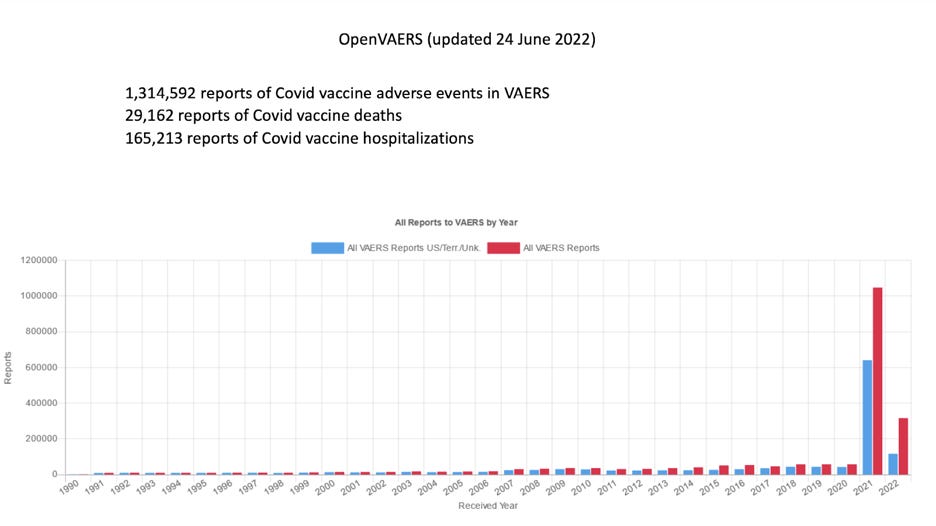
Forum: There is also confirmation of both deaths and serious complications from the vaccines, but these numbers are also ignored. Have you reviewed the data bases like VAERS [Vaccine Adverse Event Reporting System]?
Fenton: As of June 2022, we saw over 1.3 million adverse events showing in the VAERS database, a system widely accepted as flawed for underreporting. Even with these low numbers we knew that there had been about 30,000 deaths and over 165,000 hospitalizations caused by the COVID vaccines. In all previous years since VAERS began recording data, the total number of deaths reported from all vaccinations before COVID was around 10,000. So there are three times as many deaths reported from the COVID vaccine in two years, compared to all deaths from all other vaccines in the reporting over the last 30 odd years. This should be taken as an obvious signal, stopping the COVID vaccine program for reevaluation, but again these numbers are dismissed.
COVID-19 cases by immunization status, Dec. 17, 2021 - May 5, 2022. Graph by Norman Fenton.
Forum: What about the argument that this is an insignificant number compared to the millions of people who are vaccinated without reported problems?
Fenton: For the people with reactions and for those who died, it’s not insignificant. The most important questions concerning risk versus benefit haven’t been addressed, and any data questioning vaccine dangers have been successfully repressed. What we do know from some of the numbers is that there is a verifiable risk and questionable benefit. Despite what is reported in the mainstream media, respected clinical colleagues have told me there is increasingly less argument to support vaccination. There is also a ground swell of virologists saying that the newer variants are less dangerous as well. Of course, this is also not widely reported, as it would stop the push for vaccination.
Forum: This pressure for vaccination hasn’t relented, even for the youngest children. Was the trial data ever made public for use on infants?
Fenton: When it comes to vaccinating infants and children, the right kind of trials to determine safety would need years to get reliable figures. What we do have are the anecdotal reports about teens and young people who have had serious complications from the vaccine. And we can consider this information along with the known low risk of complications from having the virus for anyone under twenty. Again, risk versus benefits have not been applied.
Forum: As the pandemic seems to be subsiding, are you seeing signs that the data that you and others have analyzed will be considered in reviewing the response? Do you think there is some awakening?
Fenton: In recent weeks there has indeed been more widespread awareness that the mainstream narrative about both the lethality of the virus and the safety and effectiveness of the vaccines has been exaggerated. And as a result, in the UK for sure, we are seeing much lower take-up of the latest vaccine boosters than the previous ones. However, there is still extreme censorship relating to data on vaccine deaths and injuries — and a reluctance to even hear the stories of those people who are vaccine-injured or bereaved.
My concern is that we may never know the true long-term safety of the vaccines because there has been such a concerted attempt to eliminate the control group — those people who were never vaccinated. We are now seeing excess death increases in the most highly vaccinated countries. But in the absence of accurate or sufficient data about how many of these are unvaccinated compared to vaccinated, the mainstream narrative is suggesting every possible cause other than the vaccines.
The notion of long COVID as a major cause of problems is especially being promoted; as this strengthens the argument that COVID is debilitating and lethal and further supports the need for continued vaccination. This hypothesis could easily be tested if we had accurate data comparing long COVID in the vaccinated and unvaccinated. But we have found that no such data are being collected.
Dear David --
Robert Malone writes that you are a CHD Fellow.
Would you please bring this post to the attention of people at CHD?
This is real hard Data showing the effect of the Vax -- very hard, undeniable Data.
https://timellison.substack.com/p/high-correlation-between-vax-rate